Medication Administration Record Sheet PDF Template
Medication Administration Record Sheet PDF Template
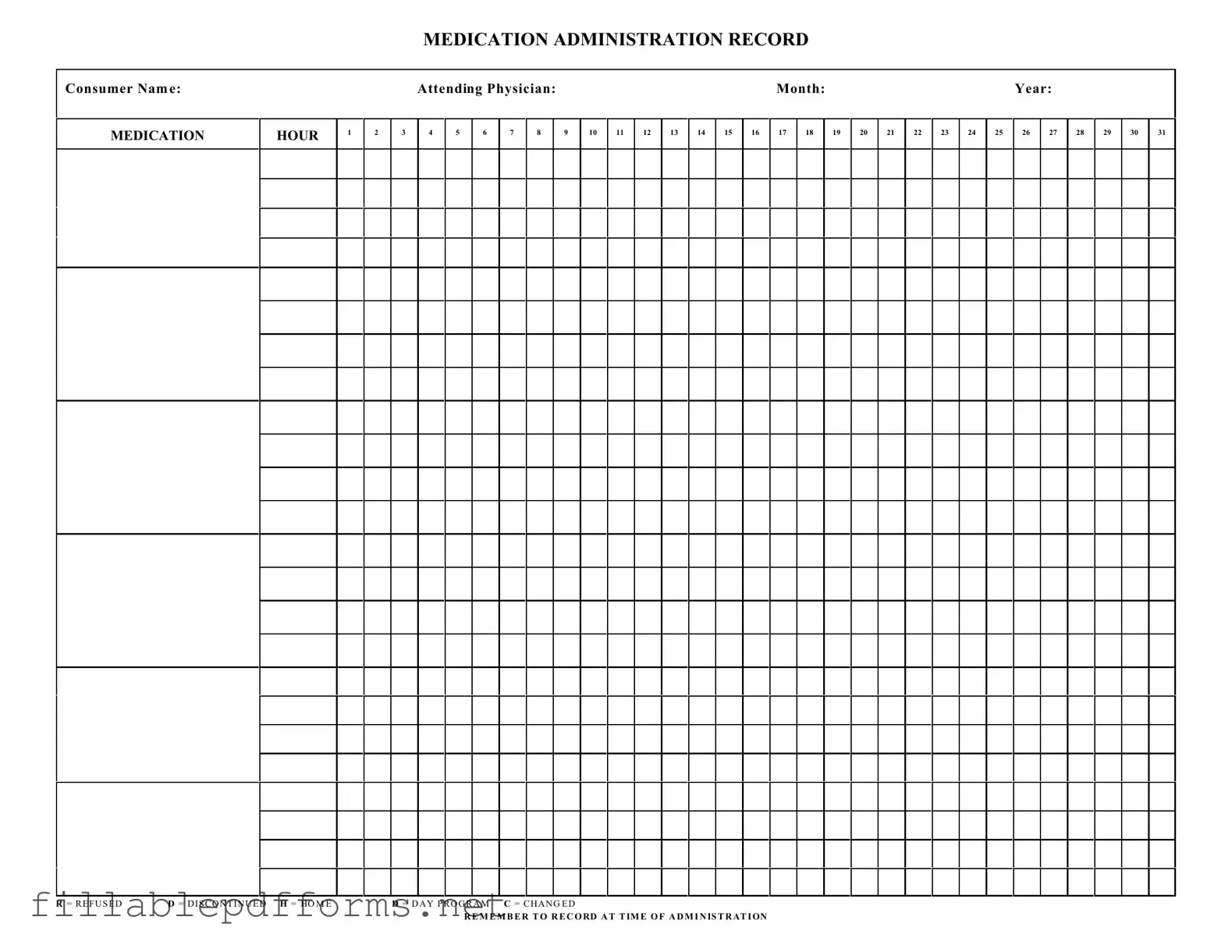
The Medication Administration Record Sheet is a vital tool in the healthcare setting, designed to ensure accurate tracking of medication administration for patients. This form includes essential details such as the consumer's name, the attending physician, and the specific month and year of record-keeping. Each hour of the day is accounted for, allowing healthcare providers to document the precise times medications are administered. The form also incorporates a system of notations, where healthcare professionals can indicate if a dose was refused, discontinued, or changed. This structured approach not only enhances patient safety but also facilitates communication among the healthcare team. By recording these details diligently, providers can maintain a comprehensive history of medication management, which is crucial for ongoing patient care and treatment adjustments. Remember, timely and accurate documentation is key to effective medication administration.
Failing to include the consumer's name at the top of the form. This can lead to confusion about who the medication is for.
Not recording the attending physician's name. Omitting this information can complicate communication regarding treatment.
Forgetting to mark the medication hour accurately. This can result in missed doses or incorrect administration times.
Neglecting to indicate the status of the medication, such as refused or discontinued. These notations are crucial for tracking the consumer's medication history.
Not recording the administration at the time of administration. This oversight can lead to errors in medication management and affect the consumer's health.
Understanding the Medication Administration Record Sheet (MARS) is crucial for ensuring accurate medication management. However, several misconceptions can lead to confusion and errors. Here are seven common misconceptions:
Addressing these misconceptions can improve the accuracy and effectiveness of medication administration, ultimately enhancing patient safety.
Completing the Medication Administration Record Sheet is essential for accurate tracking of medication given to consumers. Follow these steps carefully to ensure all necessary information is recorded correctly.
When filling out the Medication Administration Record Sheet, it is essential to follow specific guidelines to ensure accuracy and compliance. Below are some important dos and don’ts.
How to Travel With a Dog Internationally - Your pet's comfort and safety is paramount; this form is part of ensuring that during travel.
For those navigating the complexities of trailer transactions, understanding the importance of a proper document is crucial. Utilizing a well-crafted trailer bill of sale is fundamental for ensuring a smooth transfer of ownership, providing essential protection for both the buyer and the seller. For a reliable resource, consider reviewing the comprehensive Georgia trailer bill of sale for guidance on this important form.
Work Incident Report Template - Encourage an open dialogue about workplace safety through reporting mechanisms.
Filling out and using the Medication Administration Record Sheet (MARS) is crucial for ensuring accurate medication management. Here are some key takeaways to keep in mind:
By following these guidelines, caregivers can enhance the safety and effectiveness of medication administration for consumers.