Cna Shower Sheets PDF Template
Cna Shower Sheets PDF Template
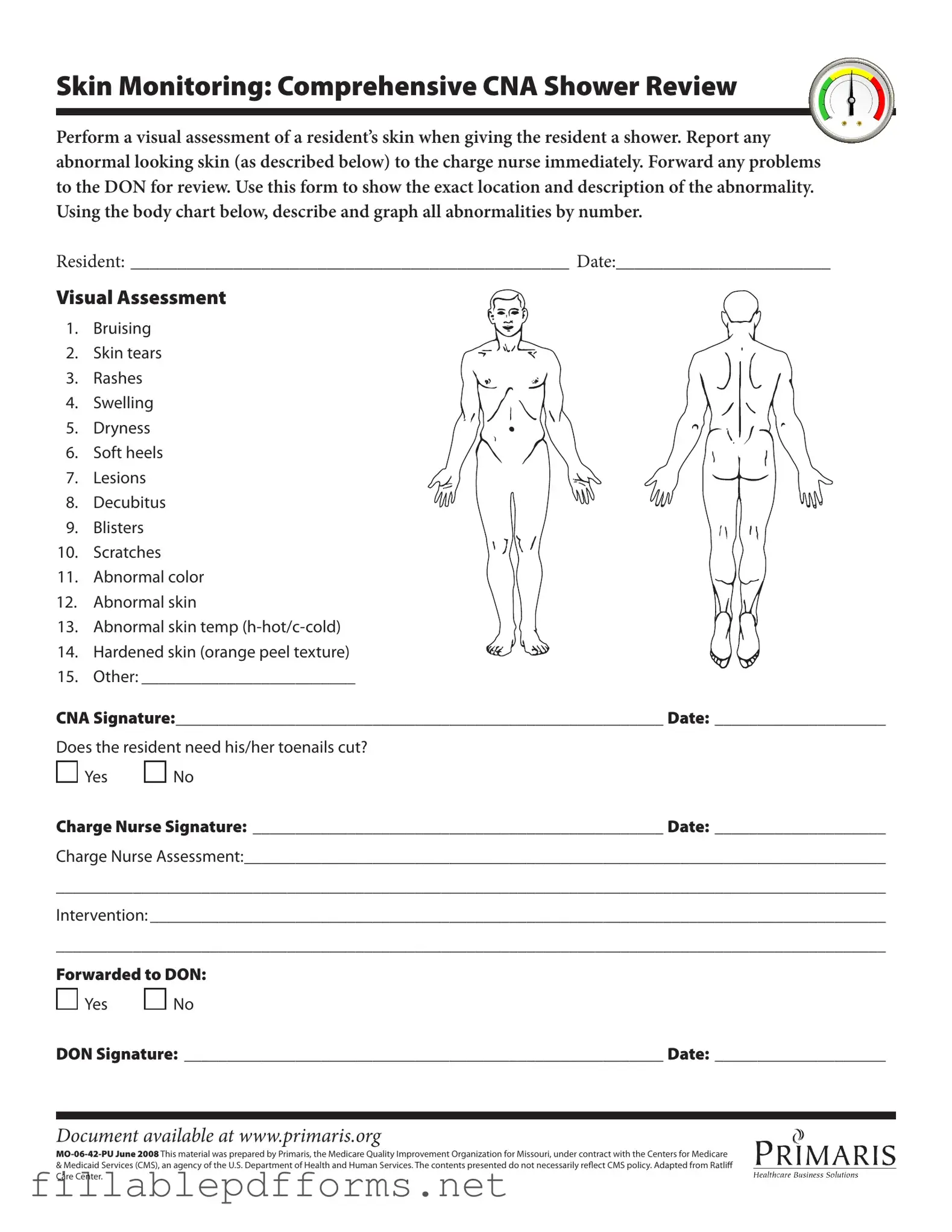
The CNA Shower Sheets form serves as a vital tool in ensuring the well-being of residents during their bathing routine. This form is designed to facilitate a thorough visual assessment of a resident’s skin while providing a shower, highlighting the importance of monitoring for any abnormalities that may arise. Caregivers, specifically Certified Nursing Assistants (CNAs), are tasked with documenting various skin conditions, such as bruising, skin tears, rashes, and other irregularities. Each abnormality must be noted with precision, including its exact location on the body, which is illustrated on an accompanying body chart. Additionally, the form prompts CNAs to assess the overall condition of the resident's skin, checking for signs of dryness, swelling, or lesions, among other concerns. Should any issues be identified, it is crucial for CNAs to report these findings to the charge nurse immediately, ensuring that appropriate interventions are initiated. The form also includes a section for the charge nurse’s assessment and any necessary follow-up actions, including forwarding the information to the Director of Nursing (DON) for further review. Ultimately, the CNA Shower Sheets form not only aids in maintaining high standards of care but also promotes effective communication among healthcare team members, enhancing the overall health and comfort of residents.
Incomplete Resident Information: Failing to provide the resident's full name and date can lead to confusion and miscommunication.
Neglecting to Document Skin Abnormalities: Skipping the visual assessment of skin can result in missed health issues that require attention.
Using Vague Descriptions: Describing skin abnormalities without sufficient detail can hinder effective communication with the charge nurse.
Not Following Up on Abnormal Findings: Failing to report abnormalities to the charge nurse immediately may delay necessary interventions.
Omitting Signatures: Forgetting to sign the form can lead to questions about accountability and responsibility for the care provided.
Ignoring Toenail Care: Not addressing whether the resident needs toenail trimming can overlook an important aspect of personal hygiene.
Understanding the CNA Shower Sheets form is essential for proper resident care, but there are several misconceptions surrounding it. Here are nine common misunderstandings:
Clearing up these misconceptions can help ensure that residents receive the best possible care and that CNAs feel confident in their responsibilities.
Completing the CNA Shower Sheets form is essential for documenting skin assessments during resident showers. Accurate and timely reporting helps ensure that any skin abnormalities are addressed promptly. Follow these steps to fill out the form correctly.
When filling out the CNA Shower Sheets form, there are important practices to follow. Here are four things to do and not to do:
Farbar Forms - Landlord responsibilities regarding maintaining property structural integrity are detailed for tenant security.
Acord 130 - Specifics about employee inclusion or exclusion in coverage must be mentioned.
The New York Motorcycle Bill of Sale form is essential for anyone looking to buy or sell a motorcycle, ensuring that the transfer of ownership is documented comprehensively. To facilitate this process and avoid any ambiguities, individuals can access the form easily at My PDF Forms, allowing for a smooth and transparent transaction that protects both the buyer and seller.
Bdsm Limits List - Assess your comfort with shaming or praise during play.
When filling out and using the CNA Shower Sheets form, it is essential to adhere to specific guidelines to ensure accurate documentation and effective communication regarding resident care. Here are key takeaways to consider:
By following these guidelines, CNAs can ensure that the documentation process is thorough and that residents receive the appropriate care based on their individual needs.